
In Beira, practical training has begun for the 20 nurses participating in the annual professional neonatal nursing course, which started last February, in the province of Sofala in Mozambique. “Formador”, as the tutors are called by the students, “can we discuss a case together? Can you tell me if I’m doing it right?”. Opportunities for discussion and growth are not to be taken for granted for those who have often been accustomed to working without adequate training, alone, in a context where challenges are many.
This is the first course of its kind in Sofala, following an initial year in Maputo. The theoretical training has been completed and the participants have now begun their practical training, which will take place at the Central Hospital in Beira and the Central Hospital in Maputo, particularly in the delivery room and the neonatal unit. This is definitely something innovative because it is the first time that there are nurses in the delivery room dedicated exclusively to newborns.
“You know, Dotora, I did a lot of things before, but I didn’t really know why I was doing them or when it was best to do them. Now I’m prepared, I know what to do and when to do it, so I make informed choices,” said Gracinda, a nurse who has been working in the Berçário at Beira Central Hospital for seven years. Irene Avagnina, a CUAMM paediatrician at Beira Hospital, reports this with satisfaction, recounting the initial feedback received from course participants: “A strong, collaborative team has been created, where people help each other and exchange knowledge and experience. It was essential to make them understand how important they are in the first moments of a newborn’s life, that their service can have a crucial impact! When they successfully resuscitated children or managed to resolve a complex situation, you could clearly see their amazement and gratification at the opportunity to really make a difference.”
A shared commitment to investing in the growth of local human resources, professional training that is part of the project “Strengthening the system of healthcare personnel training institutes and supporting the development of telemedicine”, funded by the Italian Agency for Development Cooperation and implemented with Aispo, the Community of Sant’Egidio and the University of Sassari.


“It was important that the Ministry decided to involve staff already in service. This is definitely the key to having a real impact on the healthcare system, giving operators the opportunity to grow. Despite the challenges of implementation, there has been a clear willingness on the part of the Public Institute of Science and Health to take on this commitment and to think of it from the outset as an ongoing and long-term course because it is seen as a concrete opportunity for improvement,” adds Irene. The Institute is still feeling the effects of Cyclone Idai and the economic crisis, but despite this, it remains a national reference point for professional training in nursing.
“On Mozambican Women’s Day, we got together with our colleagues. We stood in a circle, each of us wearing a capulana – a traditional Mozambican fabric worn by women, which has a strong symbolic value. We had to share a wish, the hope that each of us had for this course,‘ concludes Irene. ’At the end, the group sang a song that says: “Those who were afraid to be born, now appreciate life”.









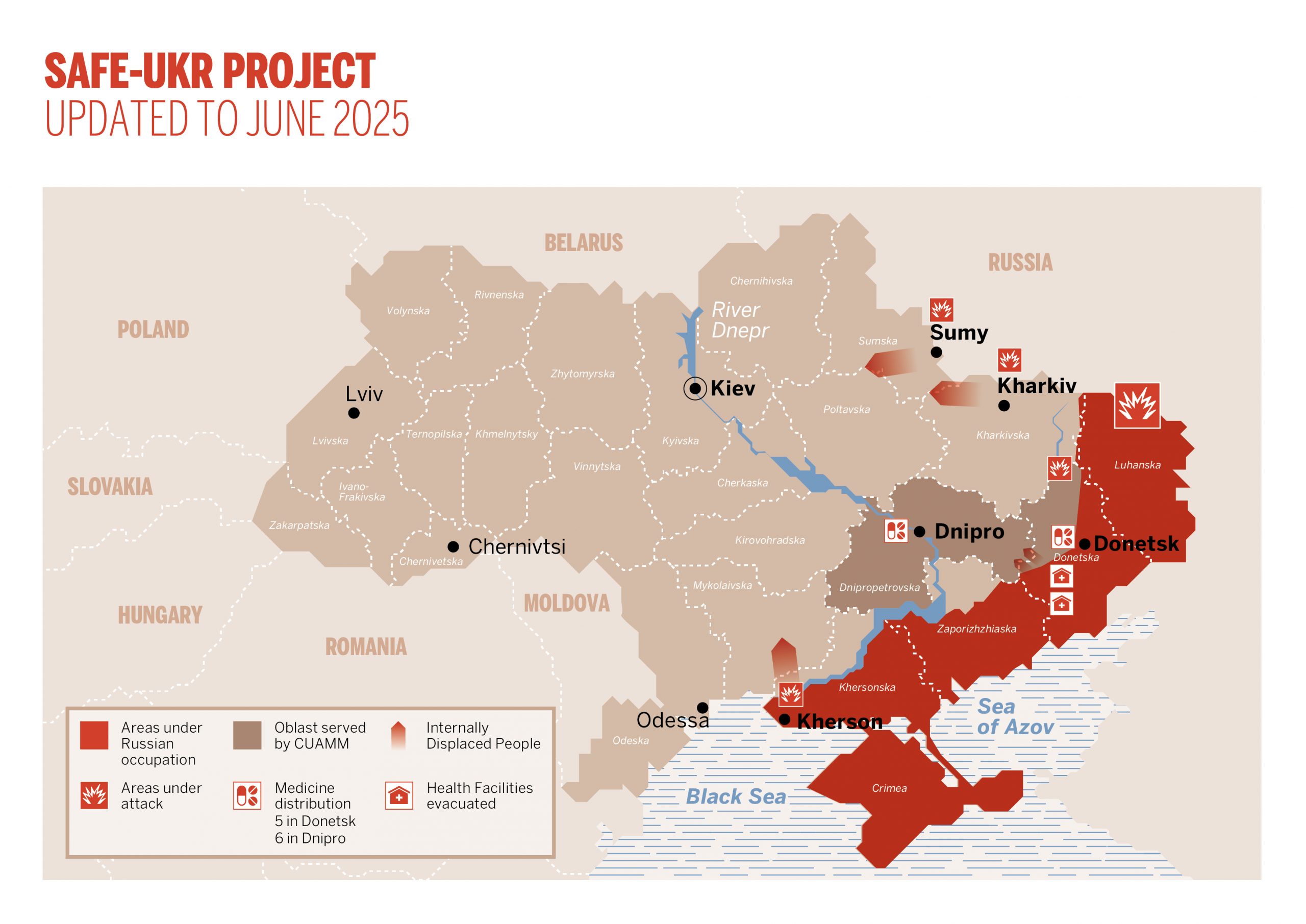 Today, as the conflict shows no signs of ending, on the contrary it becomes more intense in the Dnipropetrovsk region, the need to ensure access to care and assistance remains, as noted by Andrea Atzori, CUAMM Head of International Relations.
Today, as the conflict shows no signs of ending, on the contrary it becomes more intense in the Dnipropetrovsk region, the need to ensure access to care and assistance remains, as noted by Andrea Atzori, CUAMM Head of International Relations.



